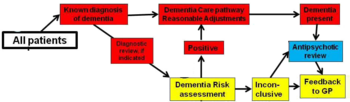
A clinical pathway is a multi-disciplinary view of the care process for a group of similar patients suffering from the same disease and with predictable evolution. While scheduling the care for a single patient is straightforward, scheduling the care for a group of patient, and under limited resources is much more complex, and software tooling might provide useful help to deliver quality schedules.
Date: 1 December 2015
Expertises
Asset
About project
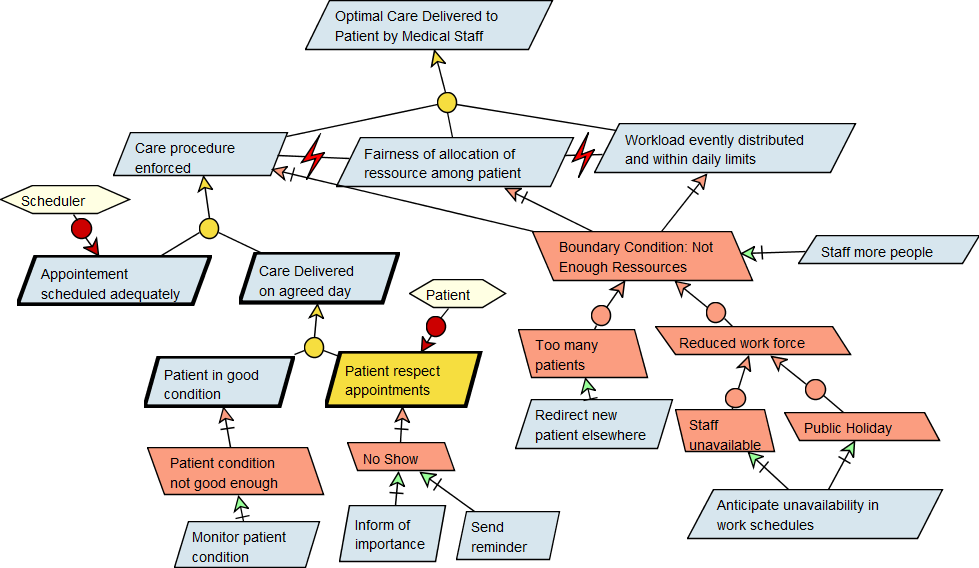
Organising care delivery is a complex taskhaving to deal with many different goals of different natures, especially in the contexte of chemotherapy pathways. In such setting, a functional goal is to be able to schedule patients in a way that must not only be feasible with respect to the resource (e.g. rooms, equipment and staff working hours), but must ensure some strict timeliness-related quality for the patient, and in a fair way for every patient engaged in the pathway. On top of this the system must be resilient to a number of adverse event such as patient failing to show or delayed for medical reasons. In order to make explicit such goals, conflicts among them and possible obstacles against them, a goal-oriented model was build (see Figure below) using a sound method developed in the field of requirements engineering. Knowing those goals their inter-relationships and how to measure them was a key prerequisite for the success of the whole project, e.g. to design procedures anticipating impacting delays, to define the optimisation strategy, to ensure the long term match of required resources.
In this context, optimization tools can provide useful tooling to organize and schedule clinical pathway. Such tool must take into account that the flow of patient is actually continuous, and that some disturbing events related either to the patients or to the medical crew might require adapting the schedule or the treatment on the fly. Such adaptation should of course not require a complete re-organization of the planning that should modify a large set of set appointments.
Software tool used so far to assist in the elaboration of such schedule are mostly manual and are typically based on spreadsheet software. Several approaches have been proposed to elaborate schedules, but they often lack some attentions to be paid to the timeliness of care, impacting care quality.
Our goal is to show that within clinical pathway, appointment planning can be driven by timing-related medical indicators. This way, the planning of each patient is compatible with his own timing constraint, and the global schedule matches the available resources, under the assumption that there are enough resources.
In our research, initiated under the PIPAS project PIPAS, we have focused our effort on the scheduling of chemotherapy pathways in oncology. Chemotherapy drugs must be delivered in several doses. To be efficient, dose deliveries must be kept within close timing. On the other hand, a minimal delay must be observed between dose deliveries to avoid damaging the patient’s health further, because of the toxicity of such treatments. If dose deliveries are spaced too widely, or if a dose is not delivered, cancer cells get an opportunity of growing again (see figure 1).
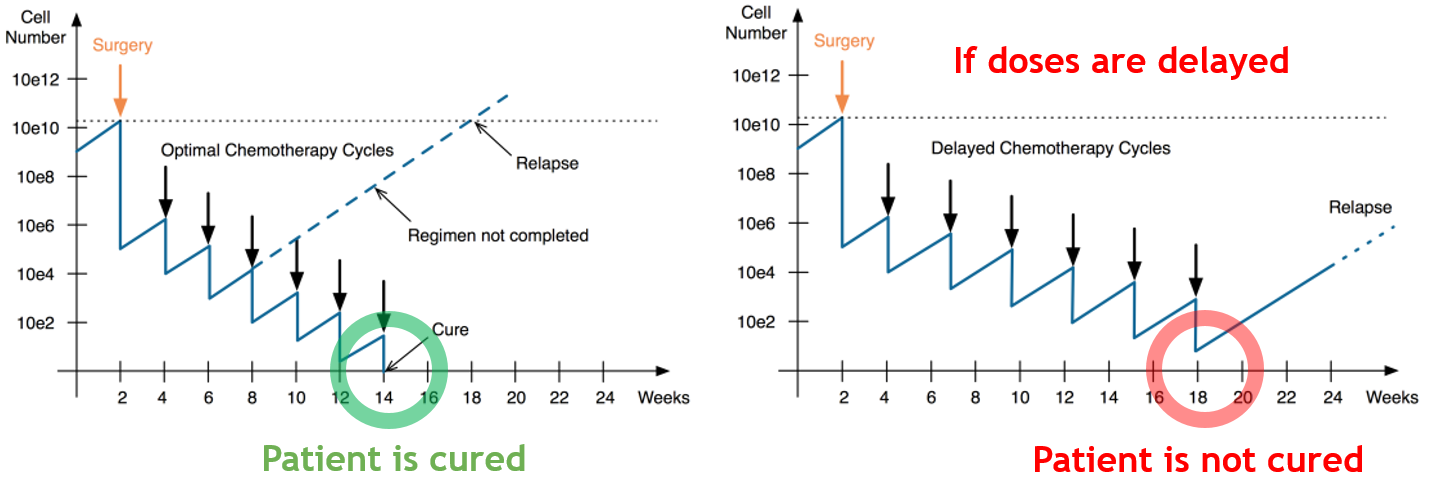
A numerical indicator has been defined to measure the timeliness quality of dose delivery, it is called the RDI (“relative dose intensity”). Its formal definition refers both the total delivered dose and the duration of the treatment. It is expressed as a percentage: 100% means that the total standard dose was delivered in standard time, 0% means that no dose was delivered. Medical research has shown for a large set of cancers that this indicator is correlated with the efficiency of the treatment in term of survival and relapse. This indicator is therefore a key metrics for scheduling
appointments in the context of chemotherapy.
We have developed a prototype based on agile methods, to evaluate the impact of optimizing appointments on the RDI of patients in order to maximize the efficiency of chemotherapy on groups of patients under restricted resource constraints. We started with a simplified model of workflow of chemotherapy. These were developed through a rigorous analysis. It includes resource constraints, and the fact that the available resource varies over time. We have developed an appointment scheduler, and a set of tools including a scenario base, a graphical user interface to manage appointments, and a simulator of patient for validation purposes. This simulator could help us validate the prototype with oncologist for various hospitals (Institut du Cancer de l’UCL, Grand Hopital de Charleroi, and UZ Leuven).
The following aspects were gradually added to our tooling, to finally get a model that is sufficiently realistic for a real-life validation:
Our goal is to maximize the RDI among the considered pool of patient. There comes the notion of what is a global objective with respect to the local objective of individual patients, and the notion of equity. We have developed two different notions of global RDI. The first one is to consider the minimal RDI among the pool of patient, so as to maximize it. Another criterion is to maximize the sum of all RDI. Our prototype is able to schedule the appointments for a pool of five hundred patients in a few seconds, and supports some interaction with the medical crew, to adjust the planning interactively.
We relied on our simulator to validate the scheduler. Thanks to our simulator, we could execute the software step-by-step, as well as simulate over long period of time, or under tight resource constraints. We had rather positive return from the medical staff about guaranteeing care quality with smart management of the available resources. The next figure is a typical example of simulation where a high RDI could be achieved for each patient.

The prototype raised ethical concerns in case resources are too scarce compared to patients, so that patients conflict for some dates. Our conclusion is that the tool should also report such situation as soon as possible to the medical staff in order for them to remedy to this situation.
Our graphical interface provides a way to the medical staff to keep a hand and a view of the situation. Some features such as a dedicated window for the oncologist when planning an appointment can also report on the current and estimated RDI, and the acceptable time frame for the patient.

By combining our Oscar.CBLS scheduling engine with visualization and simulation components, we have shown that the clinical pathway of a large pool of patients can be scheduled, based on medical, time-related, quality indicators.
A relevant question raised by doctors is it really a good idea to use an optimization tool in such critical setting? As always, the answer is not in the technology but in the way we use the technology at the system level. Clinical pathways help taking complex decisions, and our feeling is that such scheduling tool can greatly assist medical crew in their day-to-day work and anticipate any problem that can impact the quality of care.
If you want to know more on our scheduling technology, please contact us !